Dyspraxia / Developmental Coordination Disorder (DCD)
Understanding motor coordination differences from a neuroaffirmative perspective
What is Dyspraxia / DCD?
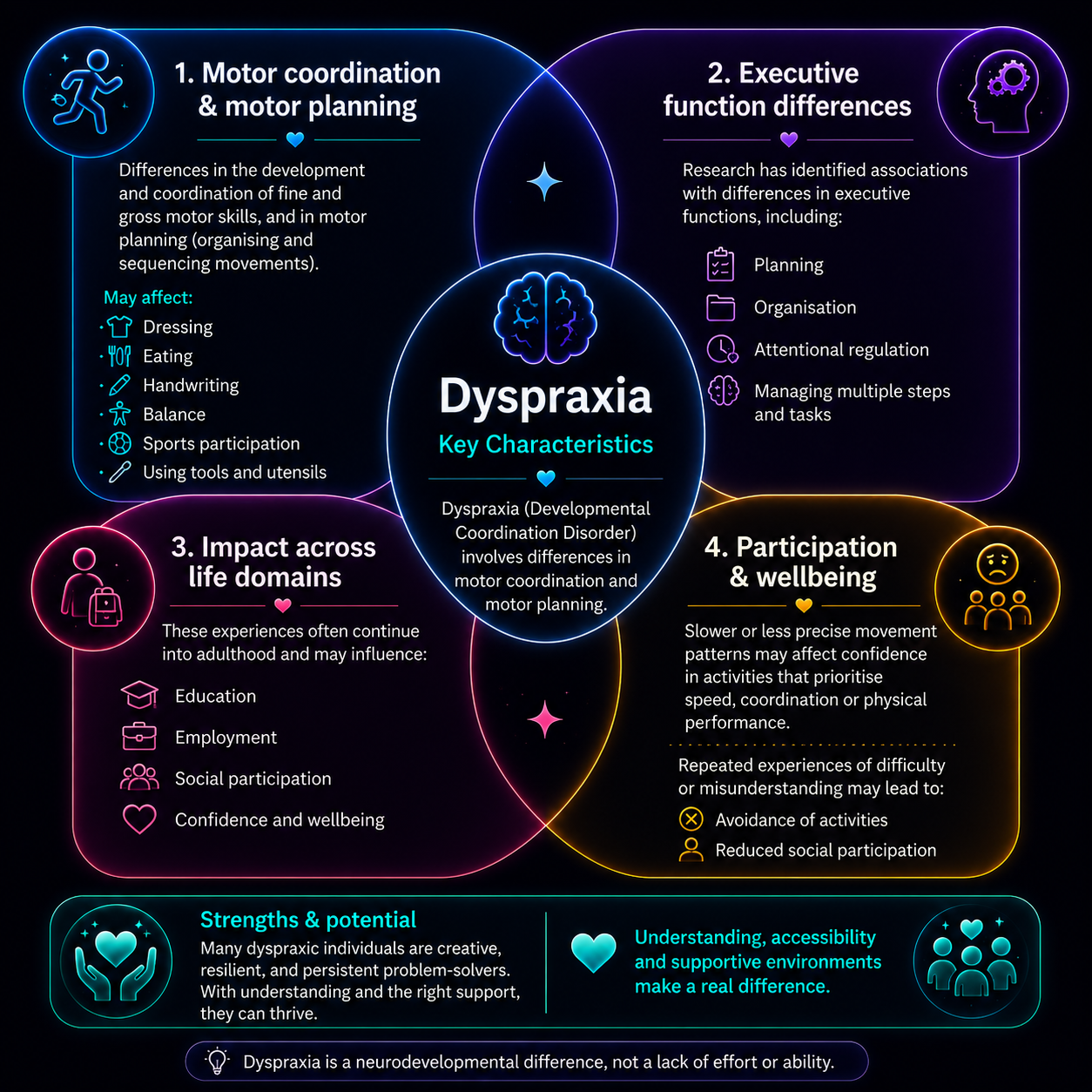
Developmental Coordination Disorder (DCD), also referred to as dyspraxia, is a neurodevelopmental difference characterised by motor coordination patterns that diverge from age-related expectations and are evident across contexts from early childhood (APA, 2013). Historically, terms such as childhood dyspraxia and clumsy child syndrome have been used to describe the same presentation.
From a neuroaffirmative perspective, dyspraxia is understood as a difference in motor planning, execution, and organisation that may interact with environmental, relational, and societal expectations. These differences can influence participation in everyday activities, including self-care, play, leisure, education, and work, as well as tasks involving fine and gross motor coordination (Lingam et al., 2014).
Dyspraxic individuals may experience motor execution as effortful, slower, or less precise, with associated challenges in planning, sequencing, and executive functioning (Leonard et al., 2015; Pedro et al., 2019). Across development, repeated experiences of misattunement, pressure to conform, or limited access to appropriate adjustments may contribute to reduced self-confidence, participation, and relational safety, rather than these outcomes being inherent to dyspraxia itself (Fitzpatrick & Watkinson, 2003; Missiuna et al., 2008).
Social participation and relationships may be shaped by the degree to which environments allow for flexibility, understanding, and inclusion, as avoidance of motor-based activities often reflects contextual barriers rather than lack of interest or motivation (Dewey & Volkovinskaia, 2018; Payne et al., 2013).
Consistent with diagnostic guidance, dyspraxia is identified where motor differences are not better explained by visual impairment or another neurological condition (APA, 2013).
Dyspraxia Strengths
Alongside clinical descriptions, neurodiversity-affirming and social model perspectives suggest that many challenges associated with dyspraxia arise through interactions between individuals and environments that are not designed for different ways of moving, learning, and participating (Armitage et al., 2017; Oliver & Barnes, 2012).
Dyspraxic individuals often describe strengths such as creativity, imagination, problem-solving, storytelling, music-related abilities, and thoughtful decision-making. Whether these characteristics are experienced as strengths or challenges often depends on context, expectations, and the availability of appropriate support and adjustments (Maw et al., 2024; Zwicker et al., 2018).
Some individuals may also experience lower confidence, reduced self-esteem, or social difficulties following repeated experiences of misunderstanding or being judged against neurotypical expectations (Caçola, 2016; Milton, 2012; Zwicker et al., 2012). Person-centred, formulation-led approaches can help understand these experiences within the context of identity, relationships, strengths, and lived experience, supporting collaborative understanding and meaningful support (Johnstone, 2018; Stricker & Gold, 1996).

A neuroaffirmative note
From a neuroaffirmative counselling psychology standpoint, distress is commonly linked to misattunement, lack of accommodations, and stigma, rather than neurodevelopmental differences and traits themselves. Neuroaffirmative practice prioritises empathetic, low-pressure approaches that reduce anxiety, honour autonomy, and create relational safety, through collaborative meaning-making and environmental adjustments to support accessibility, participation, and quality of life.
2%
severely affected
Helpful Resources & Links
Dyspraxic Adults — Community Forum
Online community forum for dyspraxic adults to share experiences and support.
https://www.dyspraxicadults.org.uk/forums/viewforum.php?f=16

Movement Matters UK
Clear information about Developmental Coordination Disorder (DCD) / Dyspraxia.
https://movementmattersuk.org/what-is-developmental-coordination-disorder-dyspraxia/
The Brain Charity — Dyspraxia
Information about dyspraxia and related conditions including apraxia and acquired brain injury.
https://www.thebraincharity.org.uk/condition/dyspraxia

Dyspraxia UK
Information and support for children and adults, including workplace assessments.
https://dyspraxiauk.com/

Apraxia Kids
Resources primarily for families of children with childhood apraxia of speech (CAS) and related conditions.
https://www.apraxia-kids.org/

Speech and Language UK — Resource Library
Family resource library covering childhood apraxia of speech (CAS), developmental language disorder (DLD), and related conditions.
https://speechandlanguage.org.uk/help-for-families/resource-library-for-families/
References
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (5th ed.). APA Publishing.
Dewey, D., & Volkovinskaia, A. (2018). Social cognition deficits and developmental coordination disorder. Current Developmental Disorders Reports.
Fitzpatrick, D. A., & Watkinson, E. J. (2003). The lived experience of physical awkwardness. Adapted Physical Activity Quarterly, 20(3), 279–297.
Leonard, H. C., et al. (2015). Executive function in children with developmental coordination disorder. Human Movement Science, 43, 56–62.
Lingam, R., et al. (2014). The burden and effect of developmental coordination disorder. Paediatrics & Child Health.
Missiuna, C., et al. (2008). Partnering for change. Physical & Occupational Therapy in Pediatrics.
Payne, S., et al. (2013). Social exclusion and children with DCD. Child: Care, Health and Development.
Pedro, D., et al. (2019). Motor and cognitive performance in children with DCD. Research in Developmental Disabilities.
Unless otherwise stated, all original images were created by Nahory HM and AQ (2019). This excludes images, graphics, or other content accessed via external websites, news articles, or signposted resources.